
Ampullary balloon dilation
10 January 2020
INTRODUCT�ON:
� �Portal hypertension is defined as an abnormal increase in the pressure in the veins that carry blood from the splanchnic organs to the liver. Clinically significant portal hypertension is defined as HVPG of 10 mmHg or more. Portal hypertension is a condition that can develop due to pre-hepatic , intra-hepatic or post-hepatic reasons. Clinical outcomes due to portal hypertension are variceal bleeding , ascites , splenomegaly and hypersplenism depends on splenomegly. Bleeding esophageal and gastric varices are major cause of mortality in patients with portal hypertension based on various causes. This case presentation purpose to let on about the management of gastric bleeding varices. We present a patient who was brought to the emergency room by black stool and bloody vomiting and detected fundal variceal bleeding on endoscopic process which was performed in urgent conditions.
CASE PRESENTATION:
� �56-year-old female patient was brought to the emergency room by black stool and bloody vomiting. Her blood pressure was 80/50 mmhg in both arms, pulse 110/min , fever:37.1 �C , glasgow coma scale was spotted 8 on first examination. Symptoms came to exist about 3 hours before arrival to emergency room. On physical examination ; mental status was confused ; orientation and cooperation was disordered. Active hematemesis was revealed. Abdomen was distended and bowel sounds were increased. Traube's space reflect dullness. On rectal examination melena was seen. On medical history ; patient was under consideration about chronic liver diseases but no certain reason was detected on studies. Existing medical records demonstrate ;chronic liver disease coherent findings and splenomegaly on abdominal tomography.
� �In her laboratory evaluation ; Albumin:2gr/dL (3.4-4.8 gr/dL) , T.bilirubin:1.25 mg/dl (0.3-1.2 mg/dl) , D.bilirubin:0.66 mg/dl (0-0.5mg/dl) , ALT:22 U/L (0-55 U/L) , AST:33 U/L (5-34 U/L) , GGT:28 U/L (9-36 U/L) , INR:1.62 , PT:22.7 sec. Hepatitis panel was non-reactive for A,B and C. Leucocyte count (103u/L):8.83 (4.5-11) , Neutrophil count (103u/L):6.42 (2-7.15) , Hemoglobin:11.53 gr/dL (12.2-16.2 gr/dL) , Platelet count (103u/L):95 (142-424). C reactive protein:12.77 mg/L (0-5 mg/L).
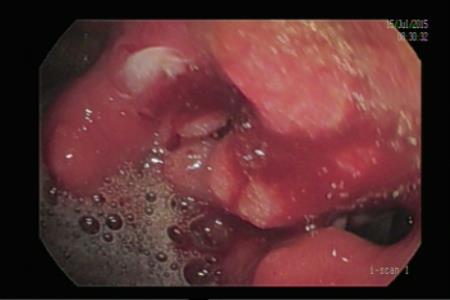
� �(IV) %0.9 NaCl fluid resusitation and octerotid infusion was started in emergency room. Endoscopic procedure was performed in urgent conditions and (F3) fundal variceal bleeding detected. Ankaferd� Blood Stopper was sprayed subsequently bleeding stopped. Afterwards Sainstaken Blackmore tube was emplaced. The patient was admitted to intensive care unit. Prophylactic third-generation cephalosporin , positive inotropic agent , (IV) fluid and octreotide infusion treatments applied. During follow up period ; bleeding took place again and another endoscopic procedure performed. First Sainstaken Blackmore tube was removed and Endoscopic Ultrasound Guided Coil and Glue Injection was applied. However, the bleeding could not be controlled. Sainstaken Blackmore tube was replaced again. Re-bleeding was attributed to high and uncontrolled portal hypertension. For this reason , transjugular intrahepatic portosystemic shunt(TIPS) operation was performed by interventional radiology and post-processing control demonstrate the porto-venous shunt. After TIPS procedure , bleeding stopped during the intensive care unit follow-up period. However, the patients unstable hemodynamic status persisted , therefore follow-up continued under positive inotropic support. The patient developed convulsion in the intensive care unit follow-up period 4 days after the first admission. The patient was consulted with the neurology clinic. Intravenous levatiracetam treatment was started according to the recommendations. However, expected epileptic seizure control could not be achieved with treatment and cardiopulmonary arrest occurred. Resuscitation failed to respond, patient was accepted as exitus.
 |
Afferent loop syndrome develops due to the obstruction of the duodeno-jejunal loop, mostly due to the recuurence of the malignancy
Read More10 January 2020
29 April 2019
27 April 2019

24 April 2019

24 April 2019
21 April 2019

3 April 2019

Related posts