Ampullary balloon dilation
10 January 2020
Background
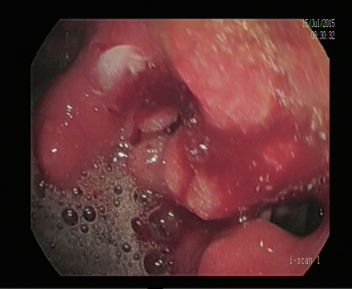
Technique
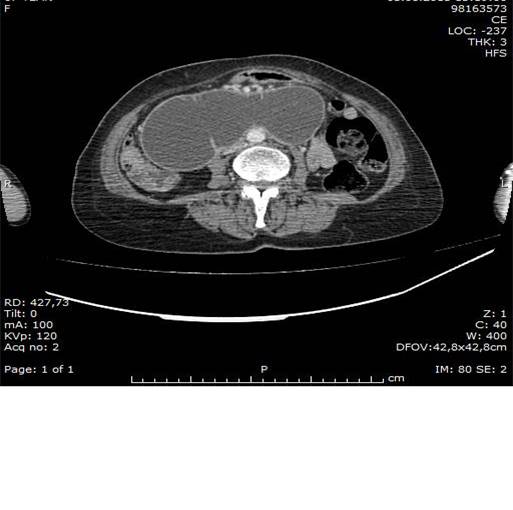
CASE




Before and After drainage
 |
 |

10 January 2020
29 April 2019
27 April 2019

24 April 2019
24 April 2019
21 April 2019

3 April 2019

Related posts