
Ampullary balloon dilation
10 January 2020
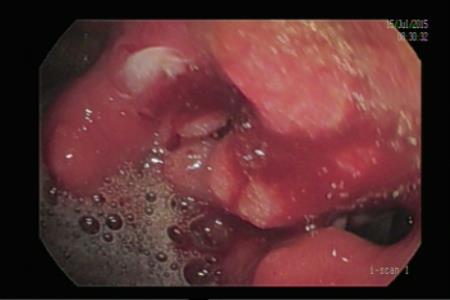
Approach to Wirsung via Stomach
Endoscopic pancreatic duct drainge is required in cases with chronic pancreatitis (CP) with main pancreatic duct (MPD) dilation.
The usual approcah is retrogarde through papilla vateri or through minor papilla in pancreas divisum. However in some cases cannnulation through these routes fail. In this cases, EUS guided approach to MPD through stomach is a viable option.
Technique:
We identify MPD from stomach with a therapeutic linear EUS scope. Afterwards preferably a 19 G G EUS needle is inserted through stomach into the MPD. We avoid vessels in between. Sometimes insertion of the needle may be difficult because of the hard pancreatic tissue due to fibrosis in CP. A brisk push may be necessary. Overshoot should be avoided. After the tip of needle is supposed in MPD, aspiration is performed to check for pancreatic fluid. We try to angle the tip towards pancreatic head, not tail. After a successful aspiration. The duct is filled with 1:1 saline-diluted contrast with the addition of a few drops of methylene blue. The syringe, 5 or 10 ml, is shaken and should have a blue color. If there is a flow into the duodenum, there are two approaches. Either withdrawal of the needle and EUS scope, duodenoscope is inserted and the flow of blue fluid is tried to be traced and cannulation with or without precut is attemped. In some previously undiagnosed pancreas divisum cases the fluid comes through the min�r papilla. However if you still fail you should return to EUS again. Because of this we try guide-wire after pancreatogram. We use 00.35 guide wire, and we try to insert it up to duodenum. This is succesful in around 50 % of the cases. Manuvering th guide wire through the needle is a daunting task and may be stuck in some cases which requires to withdraw the needle alltogether. In case it is successful, the EUS scope is withdrawn leaving the guide wire in its place. Afterwards, duodenoscope is inserted and the guide wire is identified. We generally perform sphincterotomy with taking the guide wire as a guide either with a standard sphicterotom and if cannulation besides guide wire fails with either needle knive or porcelain-tipped needle. Another approach is to grasp the guide wire and pull it through the biopsy channel and load it with sphincterotom. Fort his the best accesory is a small snare. In case you grasp it with a biopsy forcesp or grasper, it is easily disattached while withdrawing through the biopsy channel.�
In case the guide-wire cannot be inserted through the papilla and methylene blue stained fluid cannot provide successful retrograde cannulation, we dilate the tract over-the-wire with 6 F cystotom and insert a 7 F pancreatic stent and provide drainage to the stomach as it is seen in the below video case:
 |
Afferent loop syndrome develops due to the obstruction of the duodeno-jejunal loop, mostly due to the recuurence of the malignancy
Read More10 January 2020
29 April 2019
27 April 2019

24 April 2019

24 April 2019
21 April 2019

3 April 2019
Related posts