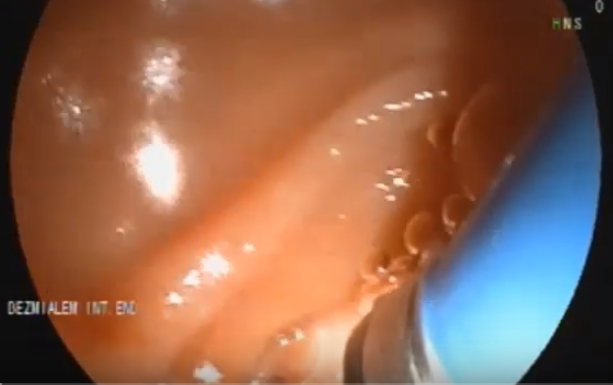
Ampullary balloon dilation
10 January 2020
Common bile duct (CBD) stones are present in 20 % of the patients with gall-bladder stones.
Considering that gall bladder stones are present in 20 % of the general population, it is a highly frequent condition.
In contradistinction to gall bladder stones, CBD stones always requires treatment becuase of very high rate of associated pancreatitis and cholangitis as well as bile duct obstruction.
Most of the CBD stones can be managed with sphincterotomy and retrieval with extraction baloon or basket or both. However in case their size is over 12 mm, or the size of the CBD distal to the stricture is narrower than the size of the stone. In this case baloon dilation up to 20 mm may be required. Up to the size of 8 mm, adjustment is not necessary. However the baloons over the size of 10 mm (large baloon dilation, LBD)should be used cautiously and their size should not exceed the size of CBD in the site of maximal dilation which means that LBD can only be used for dilated common bile ducts, and preferentially to the papillary area without associated stricture proximal to it.
In case, the retrieval is still unsuccessful, lithotripsy is required. The msot frequently used one is machanichal lithotripsy:There are several devices. However, grasping the stone in the basket is a frequent problem.
It requires a spyglass cholangioscopy device. Very recently spyglass generation 3 came to market with a better resolution in comparison to the previous ones.
Spyglass is inserted through a duodenoscope with a working channel 3.7 mm or over after sphincterotomy. Its size is 10 French. It can be inserted directly or over the guide wire. Insertion over the guide-wire is easier. After insertion the handle of spyglass is attached to the the lower end of duodenoscope handle and the guide-wire is withdrawn. Spyglass cholangioscope has an insertion channel of 2 F, right/left and up/down button. It has a water insufflation and aspiration system. An one french catheter is inserted through the working channel and the stones are fragmented with touching with the tip of the catheter and administering laser current.
Operating SOC, requires controlling two scopes (duodenoscope and cholangioscope), hence four buttons. The novice cholangioscopy users, sometimes try to operate the system by two endoscopists as it used to be in mother-baby cholangioscopes. However this approach does not work in SOC, because as its name implies it design is for one operator.
I personally hold the handle of the duodenoscope at my chest with my left arm, operate the buttons of the SOC with my left hand fingers and use my right hand for the operation of laser-wire as well as insertion and withdrawal of the SOC.
While operating the SOC, the operator should keep an eye on the position of the duodenoscope. Usually it slips to the proximal as far as stomach, if the operator, only deal with SOC. If the short position of duodenoscope is altered, the operator, first adjust it and then go on with the SOC.
 |

10 January 2020
29 April 2019
27 April 2019

24 April 2019
24 April 2019
21 April 2019

3 April 2019

Related posts