Ampullary balloon dilation
10 January 2020
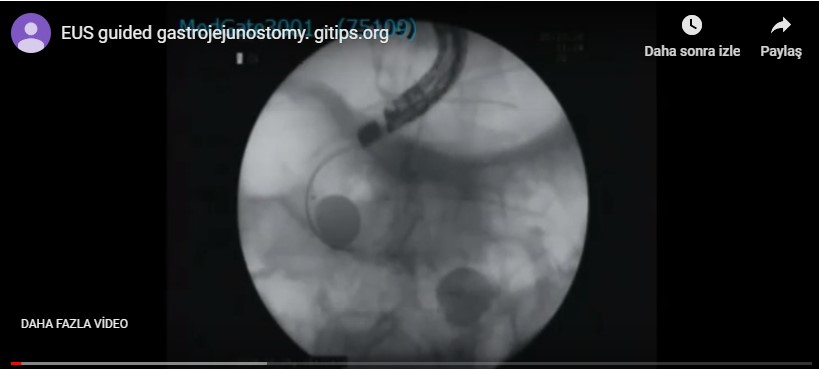
Gastric outlet obstruction is not uncommon in gastric and pancreatic carcinoma. Indeed, it happens in 40 % of advanced pancreatic carcinoma. Previously it used to be managed for palliative purposes by surgical gastrojejunostomy. It is burdensome for the patient and costly. Endoscopic stenting is the usual practice that an self expandable metallic stent (SEMS) is placed. However stent migration, tumor ingrowth and outgrowth, and impaction of food bolus are common. Very recently endosonography guided gastrojejunostomy was introduced. This is the climax of therapeutic endosonography and every center that are few has its own version, although the basics are the same. In our center we do the procedure under general anesthesia while the patients is in prone position. We first insert �a gastroscope outfitted with a double balloon overtube.
We identify the stricture and insert an ERCP catheter preloaded with a 0.035 guide-wire through the stricture. We withdraw the guide-wire and confirm that the catheter is in intestine with contrast injection. We again insert guide wire and step by step forward it to the jejunum under X-ray guidence. We insert the overtube down to the antrum and withdraw the scope, leaving the guide-wire and overtube are in their places. We then insert a prototype dedicated double baloon catheter (Micrtotech company, Nanjing, China) over the guide wire and push it into the jejunum. This step requires delicate approach and managed by negotiation with to-fro movements.��After confirmeing that the double baloon catheter is in the jejunum close to gastric corpus we inflate the baloons and withdraw the guide wire. We insert a therapeutic linear echoendoscope and inject contrast diluted 1:1 with saline with a few drops of methylene blue between the baloons. Indeed, the catheter three ports, two for the baloons and one for the space between baloons. We identify the space between baloons endosonographically and radiologically and insert a 19 G needle into this space and administer aspiration to confirm that the tip of the needle is in the right place. Afterward we slightly deflate the baloons and insert guide wire through the needle. In case the guide wire is stuck to the baloons, they are further deflated to allow the guide wire forward. We withdraw the guide-wire and and dilate the tract with 6 F cystotome. This step is usually straightforward. Sometimes we are in suspicion whether the cystotom is inside the lumen or not. In this case the guide wire is withdrawn and contrast is injected. One must cautious against overfilling. Otherwise because intestines are full with contrast, one may be confused about the place of cystotom. In case you are forced to choose another site or terminate the procedure in this stage, no serious complication happens. Sometimes we choose the another site, sometimes we terminate the procedure. In this case we place a duodenal stent, insert a nasogastric tube, administer antibiotics and allow nothing per mouth. We did not encounter any serious complication. Sometimes abodminal pain and vomiting happens. You would have CT in case you want to make sure that there is no leak.�
In case we confirm that the cystotom is in the right place. We leave the guide-wire and withdraw the cystotom. Afterwards, we either insert a fully covered biliary metallic stent (usually 10X80 mm) or, better, a lumen apposing stent. The best one is hot axios however it is too costly. In case there is difficulty in insertion, dilation with a bougie 5-8.5��F is tried before stent insertion.��After the place of the stent is confirmed with administering contrast, we finish the procedur. After 2-3 weeks, we return, withdraw the stent and dilate the tract. 15-20 mm balloon and the procedure is complete. In one patient we checked after one week: We have found that the stent was migrated into the stomach. However, the fistula was complete. We dilated with 20 mm baloon. Slight bleeding happened and we put two clips, without further porblem. In another, after two weeks, stent again was found migrated into the stomach and the fistula was almost closed. We again dilated the tract. In order of ease it may be desirable to put a few clips in the vicinity of stent after the insertion. It does not only migration, but also shows the site of insertion, in case the stent is migrated and the fistula is not apparent. In our last patient, we returned after four weeks. The stent was again found migrated into the stomach. However a well formed fistula, was present. We dilated the fistula with 20 mm ballon. An unexpected free abdominal perforation happened just adjacent to the fistula. We put an 22X100 partially covered metallic stent with 26 mm flanges and put two clips adjacent. We evacuated the air from peritonel space with a percutaneously inserted veres needle. No further problem happened. It seems that lumen apposing stents should be preffered. But as it is seen the optimal timing of stent withdrawal and optimal dilation size is still not certain as well as long-term prognosis. In case the metal apposing stents are left in situ more than three weeks, serious bleeding may happen.
 |
10 January 2020
29 April 2019
27 April 2019

24 April 2019

24 April 2019
21 April 2019

3 April 2019

Related posts